The underlying pathophysiological mechanisms of chronic insomnia

The timing of sleep is regulated by two processes:1

Homeostatic process
- Sleep pressure increases during wakefulness and decreases during sleep

Circadian process
- Drive for wakefulness increases through the day and peaks during early evening
- Active promotion of sleep occurs later in the night
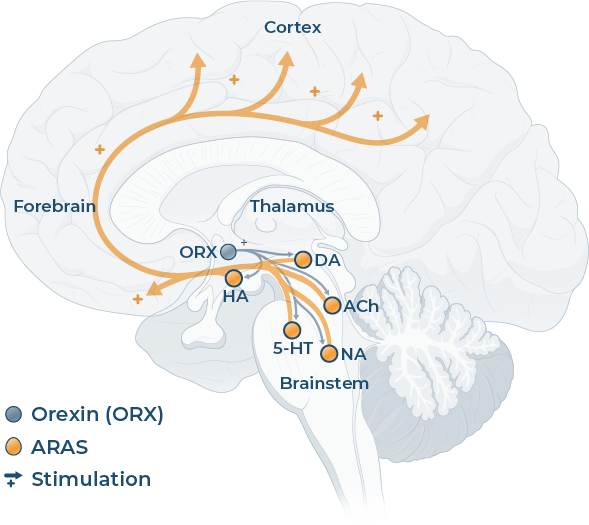
Wake-promoting systems
This image is representative of these states in the brain and the principal areas involved – it is not intended to be fully comprehensive of all brain areas involved
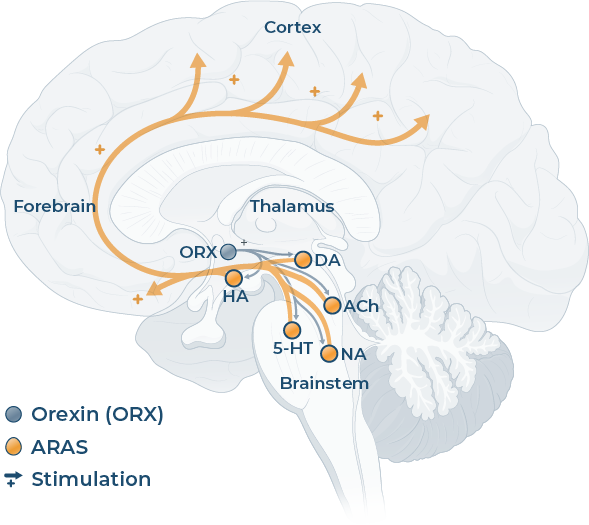
Sleep-promoting systems
This image is representative of these states in the brain and the principal areas involved – it is not intended to be fully comprehensive of all brain areas involved
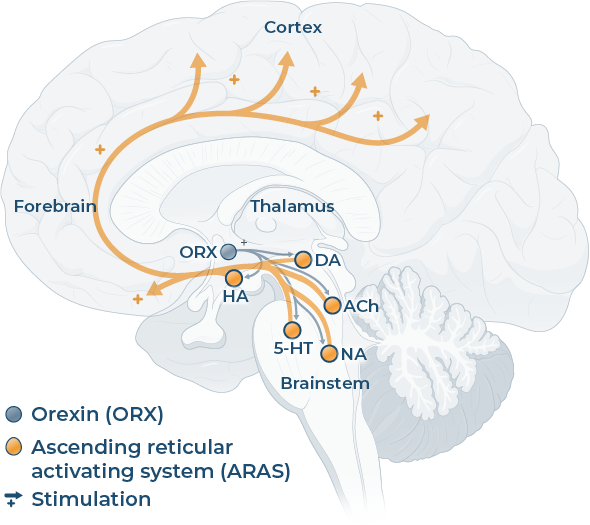
State of chronic insomnia
This image is representative of these states in the brain and the principal areas involved – it is not intended to be fully comprehensive of all brain areas involved
Quiz Summary
0 of 1 Questions completed
Questions:
Information
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading…
You must sign in or sign up to start the quiz.
You must first complete the following:
Results
Results
Time has elapsed
Categories
- Not categorized 0%
- Review
- Answered
- Correct
- Incorrect
-
Question 1 of 1
1. Question
CorrectIncorrect
Ready for the next step?
Patients with chronic insomnia may have an overactive brain at night9,10
5-HT: serotonin; ACh: acetylcholine; ARAS: ascending reticular activating system; DA: dopamine; EEG: electroencephalogram; GABA: gamma-aminobutyric acid; GAL: galanin; HA: histamine; NA: noradrenaline; REM: rapid eye movement
QUVIVIQ™ is indicated for the treatment of adult patients with insomnia characterised by symptoms present for at least 3 months and considerable impact on daytime functioning.14
This information is intended for UK healthcare professionals.
Adverse events must be reported. Healthcare professionals are asked to report any suspected adverse reactions via www.mhra.gov.uk/yellowcard or search for MHRA Yellow Card in Google Play or Apple App Store. Adverse events should also be reported to ds.safety.uk@idorsia.com
References
© NICE 2023 Daridorexant for treating long-term insomnia. Available from www.nice.org.uk/guidance/ta922. All rights reserved. Subject to Notice of rights.
NICE guidance is prepared for the National Health Service in England. All NICE guidance is subject to regular review and may be updated or withdrawn. NICE accepts no responsibility for the use of its content in this product/ publication.
- Della Monica C, Dijk D J. The external and internal factors that influence a good night’s sleep. Physiol Soc 2018; doi:10.36866/pn.113.36
- Saper C B, Scammell T E, Lu J. Hypothalamic regulation of sleep and circadian rhythms. Nature 2005;437(7063):1257-1263
- Philips A J K, Robinson P A. A quantitative model of sleep-wake dynamic based on the physiology of the brainstem ascending arousal system. J Biol Rhythms 2007;22(2):167-179
- Scammell T E, Winrow C J. Orexin receptors: pharmacology and therapeutic opportunities. Ann Rev Pharmacol Toxicol 2011;51:243-266
- Brisbare-Roch C, Dingemanse J et al. Promotion of sleep by targeting the orexin system in rats, dogs and humans. Nat Med 2007;13(2):150-155
- Saper C B, Chou T C, Scammell T E. The sleep switch: hypothalamic control of sleep and wakefulness. Trends Neurosci 2001;24(12):726-731
- Buysse D J, Germain A et al. A neurobiological model of insomnia. Drug Discov Today Dis Models 2011;8(4):129-137
- Riemann D, Nissen C et al. The neurobiology, investigation and treatment of chronic insomnia. Lancet Neurol 2015;14(5):547-558
- Nofzinger E, Buysse D J et al. Functional neuroimaging evidence for hyperarousal in insomnia. Am J Psychiatry 2004;161(11):2126-2128
- Riemann D, Spiegelhalder K, et al. The hyperarousal model of insomnia: a review of the concept and its evidence. Sleep Med Rev 2010;14(1):19-31
- Roch C, Bergamini G et al. Nonclinical pharmacology of daridorexant: a new dual orexin receptor antagonist for the treatment of insomnia. Psychopharmacology (Berl) 2021;238:2693-2708
- Scammell T E, Winrow C J. Orexin receptors: pharmacology and therapeutic opportunities. Annu Rev Pharmacol Toxicol 2011;51:243-266
- Morin C M, Drake C L et al. Insomnia disorder. Nat Rev Dis Primers 2015;1:15026
- QUVIVIQ™ Idorsia Pharmaceuticals Ltd, Summary of Product Characteristics
UK-DA-00654 | Date of preparation: September 2025